Governor visit


Governor visit
There is a wide variability in sexual function as men grow older; however a gradual decline is normal.
After treatment for prostate cancer, your sexual function can be affected. This information describes what may happen and why, and what is available to assist you. Not all aspects of male sexual problems are covered here – just the common ones you may encounter after treatment.
When a man has trouble gaining and sustaining an erection, doctors call this erectile dysfunction or ED. Many factors can prevent normal sexual function and one of the most important is simply growing older! But others are diabetes, smoking or a history of smoking, high alcohol intake and some medications. Emotional or psychological stress can also cause a decline in sexual activity. Many men have a combination of factors, so there is a wide range in sexual function as men grow older.
Prostate cancer treatment is an additional negative influence. Men who had frequent sexual activity before their diagnosis and treatment are more likely to continue this after treatment than men who were only sometimes sexually active. Men who had weak erections before treatment are likely to have weaker or no erections afterwards.
The prostate cancer itself rarely has a direct effect on reducing erectile function. It is the treatment that causes the main impact.
Drugs called PDE5 inhibitors can help men achieve an erection (see Table 1) or better quality erection. These are not aphrodisiacs (i.e. they do not increase sex drive). They work by improving blood flow to the penis.
Direct penile stimulation is required to stimulate an erection when using these drugs. If the medication doesn’t work at the first attempt, it may be worth retrying on a regular basis, say every week or two. Men on hormone treatment may also be helped by the PDE5 drugs, but often their sexual desire is low.
One theory suggests that taking a low dose of the tablets daily (e.g. Cialis, 5 mg per day) as a ‘maintenance regime’, gives you the best chance of return of erectile function. In addition, to test whether you will get a response on demand, you can take a higher (standard) dose.
Table 1: PDE5* inhibitors (medications that assist erections)
| Viagra (Sildenafil) | Cialis (Tadalafil) | Levitra (Vardenafil) | |
|---|---|---|---|
| Taken as ‘Maintenance’ Dose | Low | Low | Low |
| How often to take | Every day or every second day | Every day or every second day | Every day or every second day |
| Taken as a ‘Booster’ Dose | Standard | Standard | Standard |
| Approximate time to be taken before intercourse | 20–30 minutes | 30-45 minutes | 20-30 minutes |
| Time during which intercourse may still be possible | 2 hours (possibly 4 hours) | 36 hours | 4-5 hours |
* Phosphodiesterase Type 5
Cost
These drugs are not subsidised by the Government Pharmaceutical Benefits Scheme, so cost may be a limiting factor. Current (2011) costs for four full-strength tablets are:
Private health funds may provide some assistance.
There are side effects: Check with your doctor!
Men taking regular nitrate medication (e.g. anginine) for a heart condition must not use PDE5 medications as the risk of low blood pressure and even sudden death is increased. Your doctor will advise you on your risk or may recommend you seek advice from a heart specialist. Sexual activity is a form of exercise and heart attacks are more likely to occur during exercise than otherwise.
Headaches, facial flushing, indigestion and visual disturbances (not reported with Cialis) may be experienced by a few men. Muscle aches can also occur and may be troublesome enough to cause you to stop the drug.
A small number of medications taken at the same time may increase the risk of these side effects (e.g. the antibiotic erythromycin and antifungals such as ketoconazole).
Other products and ways of taking them will be made available in the future.
Injection therapy
Direct penile injections are the most effective form of therapy to achieve erections after a radical prostatectomy. A drug is injected each time an erection is required – this occurs without any direct sexual stimulation – it is a chemical response. Caverject Impulse (alprostadil) is the most commonly available. As with PDE5 inhibitors, it is not supported by the PBS scheme.
Start by injecting small doses (e.g. 2.5–5 micrograms) and then gradually increase the dose until a satisfactory result is achieved. This reduces the risk of one of the uncommon side effects – a painful prolonged erection, called priapism. Any erection lasting more than 4 hours with this type of medication requires prompt medical intervention, as priapism can permanently damage erectile function. Some doctors prescribe a tablet to help deflate the erection should it last for 3 hours or more, or be painful (e.g. pseudoephedrine 60–120 mg orally).
Most doctors recommend a maximum of three injections per week because more frequent use may lead to scarring within the penis. Scarring can lead to a bend in the shaft of the erect penis. The correct technique of injection therapy can be learned by most men, provided their eyesight and dexterity are reasonable.
Other injectable medications may be used, some in combination. All rely on a relatively normal blood supply to the penis; injection therapy can fail if this is inadequate.
Caverject Impulse is in a powder form that can be stored or transported at room temperature. When required it is mixed to a solution in the syringe. Other agents usually require refrigeration to store.
There are four parts to normal sexual function in men – sex drive (also called libido), erection, ejaculation (emission of fluid) and orgasm.
What causes sex drive?
At puberty, the brain increases production of hormones that stimulate greater production of testosterone by the testicles. Testosterone is the main hormone responsible for the development of male sex organs and sexual behaviour. When testosterone levels drop, sex drive diminishes.
This occurs naturally with ageing, but may also occur with illness, some commonly used medications and with hormone treatment for prostate cancer.
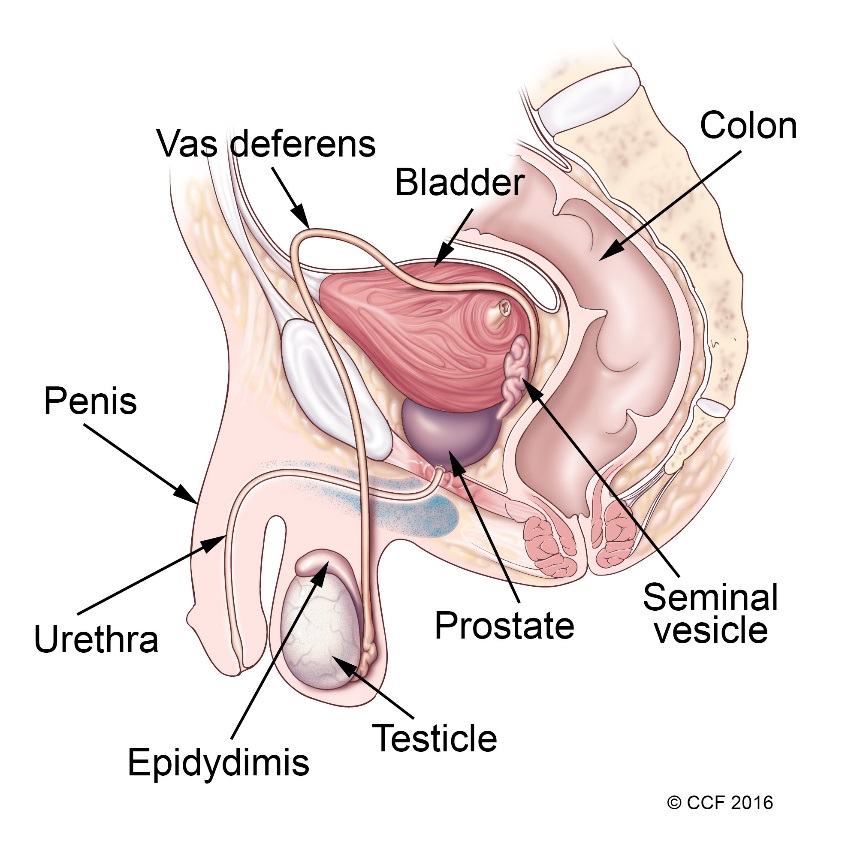
Figure 1: The male reproductive system
What happens when you have an erection?
The penis has two main chambers (the cavernosal bodies) that fill with blood when a man is sexually stimulated. This happens when nerves in the penis release a substance that causes the smooth muscle of the blood vessels (the arteries) to relax. This causes the cylinders to dilate as blood is pumped in. The penis elongates, shutting off the veins so that less blood leaves the penis than enters it. This continues until a full erection is achieved.
After ejaculation, the nerves stop releasing the muscle-relaxing substance, more blood leaves the penis than enters it and the erection subsides.
Healthy nerves and healthy blood vessels are important for erections. The nerves necessary for erections are separate from those involved in the skin sensation from the penis and those involved in orgasm.
Lifestyle factors can affect your sexual function just as they can affect your heart and general health. Not smoking, avoiding excessive alcohol intake, eating a healthy diet and exercising regularly will help improve both your fitness and your sexual function.
What happens during ejaculation?
Sperm are produced in the testes and mature in a structure close to the testes called the epididymis. Sperm are then stored in structures close to the bladder called the seminal vesicles (Figure 1). During ejaculation, semen, which contains sperm and fluid from the prostate and seminal vesicles, is propelled into the urethra (urine tube). During ejaculation, pressure builds up in the prostate region, a muscular valve at the bladder outlet closes, blocking the outflow of urine. Semen is propelled out of the penis as the pelvic floor muscles relax and contract.
What happens during orgasm?
Orgasm mainly happens in the brain and has little to do with the prostate.
As long as normal skin sensation is intact, orgasm can occur even in the absence of an erection and without ejaculation. This is a key reason why enjoyment from sexual activity can be maintained in most men after prostate cancer treatment. The common exception is men receiving hormone treatment. Hormone treatment removes the action of testosterone, frequently causing a loss of libido (sexual desire) as well as erectile function.
The prostate is not necessary for erections to occur. It adds secretions to the ejaculate, which help the sperm to survive. However it does not control the ability to have an erection.
Nevertheless, structures that are important to erectile function lie close to the prostate and can be damaged when the prostate cancer is treated. A series of fine nerves which, when active, trigger an erection, lie in bundles just next to the prostate. During sexual arousal, small blood vessels expand in order to deliver enough blood to increase the pressure in the cylinders within the penis.
Prostate cancer treatment such as radiotherapy or radical prostatectomy can damage both nerves and blood vessels near the prostate.
It is not necessary to achieve erection or penetration in order to achieve orgasm! Natural erections can improve for up to 4 years after a radical prostatectomy.
What happens after a radical prostatectomy?
This operation removes the prostate and seminal vesicles. Initially the focus is on urinary control (continence), as the nerves and muscles that help control urination also lie close to the prostate, and can be affected.
Erections
A man will normally lose the capacity to have erections immediately after the operation, however with time (several months), there is usually some return of erection strength.
In part, the return of erections depends on the extent to which the nerves that lie close to the prostate could be spared during surgery. This in turn depends on how far the cancer extends into this area and is a choice that the surgeon can make only at the time of surgery. To spare the nerves and also leave cancer behind would defeat the purpose of the operation. If it is considered safe to do so, nerve sparing (preserving) techniques are usually used to avoid damaging these nerves.
It is helpful to use oral medications (taken by mouth) such as Viagra, Cialis or Levitra and/or penile injections to cause erections early after the operation (within days or weeks). This keeps the erectile tissue working and hastens the return of unassisted erections. Some men are advised to take these tablets in low doses prior to surgery, but this is not widely recommended yet.
You may be advised by your doctor to ‘give it time’. After surgery your body needs time to heal. Erections may return gradually. The strength of the erection you may have 4 months after surgery is not necessarily the same as the one you’ll have 2 years later. Many men experience improved natural erections over time with continued improvement reported for up to 3 years postoperatively.
After a radical prostatectomy, the stimuli that caused an erection in the past may not be as effective. Different types of stimulation may be needed. Visual stimulation may not be as important as direct (hands on) stimulation of the penis. No damage to the operation site can be done through experimenting. If you have a partial erection, go ahead and attempt intercourse – vaginal stimulation may encourage further and better quality erections. Continue with sexual relations even though erections may not occur. Don’t wait for the time when they ‘just happen’.
Dry ejaculation
After the operation, because the prostate and surrounding structures have been removed, at ejaculation, you don’t usually produce any ejaculation fluid. This is called a ‘dry ejaculation’. It is possible that some urine will be lost during an ejaculation sensation, but it is not harmful.
Shortening of the penis
When there is less stimulation of the penis and the nerves and blood vessels are not working as well as before the operation, the penis appears shorter in its flaccid (floppy) state. This can be distressing to some men. As recovery progresses, the penis will usually start to look more as it did before the operation. Nevertheless, it is generally accepted that in the erect state, the penis is about 10% shorter in the long term, and this can be a concern for some men. The penis appears ‘retracted’ into the body. This can be exaggerated if there is significant weight gain.
What happens after radiotherapy?
After radiotherapy, sexual function is not usually affected in the short to medium term. Several years after radiotherapy, erectile function typically declines gradually. This is thought to be due to the progressive damage to the nerves and small blood vessels near the prostate that are important for erections. It is reported that brachytherapy to control prostate cancer has a lower risk of erectile dysfunction when compared to external beam radiotherapy (see Mr PHIP No. 3) or surgery. Intensity modulated radiotherapy is a newer technique that may reduce damage to healthy tissues adjacent to the prostate.
Remember also that ageing itself has a dampening effect on sexual function. Ejaculation fluid is often maintained after radiation treatment, but may diminish over time (usually a few years).
What happens after hormone therapy?
Control of prostate cancer using hormone treatment usually results in reduced testosterone and as a result, sex drive will be diminished for most men. However, continuation of simple physical expressions of love and concern between you and your partner can be very important in the ensuing years.
PSA tests are used to monitor cancer control after treatment for prostate cancer.
Introduction
For more than 90% of men, life continues uneventfully for many years after their treatment for localised prostate cancer. Normally there is a program of monitoring to ensure the cancer has not returned and we will describe that in this information sheet. The months and years after your treatment for localised prostate cancer are a time when it is important to improve your overall health as this can affect your outcome for prostate cancer. We give you tips on how to do this as well as to avoid unnecessary worry.
Hormone treatment controls cancer growth by reducing the effects of male hormones.
Introduction
Hormone treatment is the major treatment option for cancer that has spread beyond the prostate region or has recurred following initial treatment. It is also sometimes used with radiotherapy for the initial treatment of high risk prostate cancer. Here we describe what hormone treatment is, its effects and the long term outcome.
What is the male hormone and what does it do?
Male hormones (also called androgens) are important for the development and functioning of the male reproductive system. Men rely on normal levels of male hormones to have adult sexual function and fertility. The level of male hormone in the body is precisely controlled by several factors, the main one being the normal secretion of stimulatory hormones from the hypothalamus and the pituitary gland, two structures at the base of the brain. Testosterone is the principal male hormone. It is released from the testicles and is important for prostate growth. Both normal and cancerous prostate cells are stimulated to grow in the presence of male hormones.
What is hormone treatment?
Prostate cancer cells that have left the prostate and are growing in other areas of the body (metastases) are stimulated to grow by male hormones. A common treatment for metastatic prostate cancer is to lower the levels of male hormones in the body to control this growth. Prostate cancer cells typically die when the hormone levels are lowered. Unfortunately, not all prostate cancer cells die, and with time, often several years later, the cancer growth returns. Nevertheless, men receiving hormone treatment may get good cancer control and a symptom-free life for many years.
Hormone treatment is also called androgen ablation or androgen deprivation therapy.
The removal of male hormone or its effects means that a man will experience changes in the way he feels, his attitudes and his sex life. While this can be distressing, and it means communication with your partner is particularly important, it does not change who you are. It does not change your identity as an individual and your ability to direct your own life. Some men feel a need for a change in focus in their lives at this stage, and they may take up activities that are more meaningful to them. According to these men, the years that follow can be rewarding and productive.
You may notice changes in energy levels and sexual interest.
The time immediately following diagnosis of prostate cancer is a difficult one for many men and their families. This is partly because at the same time as coming to terms with a potentially life threatening disease, a choice needs to be made about treatment. This information describes ways men can work through the decision, and gives an outline of the main treatment options for localised prostate cancer (cancer that has not spread beyond the prostate region). Treatment options for more advanced cancer are given in Mr PHIP No. 4 and 5.